The majority of interventional cardiologists – 80-85 percent of them -- still use the traditional angiogram technique that involves the injection of contrast material into blood vessels followed by an x-ray to capture images needed to plan an interventional procedure. The other 15-20 percent augment with catheter-driven imaging devices to view arteries from the inside to guide their intervention. Until recently, these cardiologists have had only two imaging modalities to choose from: Intravascular Ultrasound (IVUS) or Optical Coherence Tomography (OCT). IVUS and OCT each come with their own set of advantages and disadvantages, so when a cardiologist chooses one over the other, it creates trade offs.
Conavi Medical recognized that limited imaging choices provided an opportunity for innovation, especially since interventional procedures are on the rise -- coronary interventions alone have now reached a high of four million procedures per year. The market opportunity was two-fold: 1.) convert non-users of imaging systems into users and 2.) create a new imaging system that would combine the best of the two existing modalities so that physicians, and their patients, wouldn’t need to compromise.
Interventional imaging choices
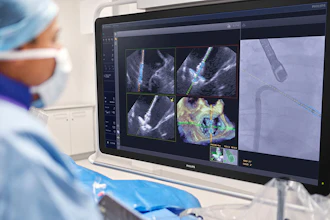
Interventional imaging allows a physician to view a patient’s vascular system via images captured inside the vessel, to determine artery size, assess lesions and calcium build up, and understand overall extent of disease. Imaging allows the physician to craft a treatment plan including selecting the appropriate stent size, ensuring the stent is placed and expanded correctly, and determining if any pre-stent vessel preparation is needed. Intravascular imaging also provides for more precise interventions that studies show result in a 50 percent reduction in adverse events after one year.
- IVUS is the most commonly used imaging system, preferred by 70 percent of interventional imaging users. IVUS provides a 5-6mm depth penetration for a good overview of a vessel, without the need to use contrast to clear blood. It can accurately size the artery (especially useful in larger arteries such as the Left Main) and assess the presence of calcium. However, it lacks resolution which can make it challenging to assess calcium thickness (important for planning vessel preparation), identify dissections, and ensure the stent is properly apposed against the vessel wall and well expanded.
- OCT is used by only 30 percent of interventional imaging users, potentially because it only provides images at a depth of 1.5-3mm, which limits the use in larger vessels. Also, OCT requires a contrast flush to acquire an image, so workflow and contrast usage concerns are another barrier. Yet OCT images have 10 times greater resolution than IVUS. OCT can also accurately assess the mechanism of stent failure, allowing the physician to plan appropriate strategies, and it is ideal for use in assessment after stent implantation.
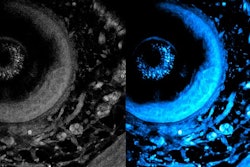
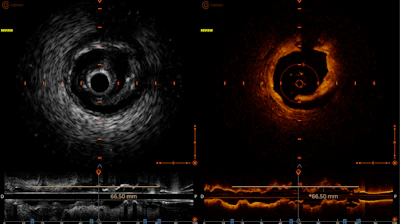
- Hybrid imaging, which combines IVUS and OCT, allows physicians to properly size vessels, assess disease, accurately identify the failure mechanism of in-stent restenosis (when a stented artery narrows or becomes blocked again, which is the most common cause of stent failure), and quickly diagnose the presence and location of calcium while measuring its thickness and arc. This insight comes from viewing high-quality, real-time images of two points of view at the same time, which are more easily interpreted. This enables physicians to choose the most appropriate therapies and more quickly determine if a therapy was effective, particularly in complex disease cases. The IVUS beam contributes to safe pre-screening of lesions for determining the best interventional strategies and OCT is most useful after intervention for optimizing treatment and managing any dissections that were created during the procedure.
The dual-imaging innovation team and what it accomplished
An interventional cardiologist in Canada had originally identified the need for the existing interventional imaging beams to come together, in a single catheter, combining the best of both modalities. IVUS and OCT were integrated into one imaging “head” with two beams that perfectly align and are co-registered (overlap) to capture images of the same part of the inside of a vessel, from two different perspectives, at the exact same time. This innovation eliminated the need to align post-processing images after acquisition by allowing physicians to accurately visualize the images in real time.
The innovation became the first generation of the Conavi Novasight™ Hybrid System, which received 510k clearance in 2018, Health Canada clearance in 2019 and was approved for use in Japan in 2020 and China in 2023. More than 300 human cases using the system have happened in North America at a handful of early-adopter hospitals. Conavi used the first generation of its system to prove its efficacy, safety, and functionality, and introduce and demonstrate the value of hybrid imaging to the interventional cardiology market. Its early learnings identified the need to make the system more robust, increase its reliability, and optimize its useability in the operating room.
When developing the next generation of its system, Conavi also hoped to discover new opportunities to gain a wide competitive edge in dual-beam imaging by adding new features and tweaking the design to be more scalable and repeatable for mass manufacturing as the product gains further adoption around the world.
To do this, Conavi engineers collaborated with Minnetronix Medical engineers, who were tasked with bringing the original product to the next level.
- Imaging quality and speed: Working together, the team discovered a way to bring the 40 MHz IVUS frequency up to high-definition levels while taking into account the higher sensitivity and any additional artifacts and noise. They also improved the final images by paving the way for imaging signals to remain clear as they traveled throughout the system -- from cameras in the catheter to the main console. It concentrated on setting a new standard for image quality by enabling the system’s motors, which used a slip ring, to rotate the two overlapping beams at a speed of 140 tiny rotations per second, speeding the capture and delivery of signals to the console, where they are clearly rendered onto a screen.
- Software and hardware features: The team enhanced the system’s software and hardware to make it able to be seamlessly integrated into the user’s workflow and improve its useability. For example, design enhancements now allow the Patient Interface Module (PIM) to be outside of the sterile field. The PIM, which was one of the most technically challenging parts of the new design, is now designed so that it doesn’t need to be put “on the table,” where it can get in the way and must be protected from fluids. It is now attached to the bed, with an extended catheter to reach the patient.
- Catheter deliverability: Conavi redesigned the catheter to reach deeper into the most challenging lesions, important for assessment of complex coronary diseases. To have the pushability and general deliverability improved, the catheter needed to be strengthened to improve reliability and protect against breakage while maintaining image quality.
- Design for manufacturability: The design stage, especially for second-generation complex medical devices, is the perfect time to review the manufacturing challenges of a gen-one build and find opportunities to redesign elements to make the product more manufacturable. The team discovered design enhancements and component selection changes that would reduce manufacturing variability of the next-gen Novasight which would increase its robustness and reliability. When variability is reduced, there are fewer costly stops and starts on the production line. One design for manufacturing (DFM) change example was swapping out fiber as a connector with a more reliable material which would reduce service calls about the product when it was out in the field. Minnetronix development and mechanical engineers made sure they understood all the requirements for the evolved product -- increased mechanical stability, minimized rotational balance, noise reduction. and speed and quality of imaging -- and derived tolerances from that knowledge. Typically, the development period between first and second generations is the greatest opportunity to not only find ways to add features, but also make changes and investment choices that will ease scalability and reduce costs down the line.
The future of dual-beam imaging
Conavi is currently educating physicians and hospital decision-makers on the benefits of dual-beam imaging to increase adoption and eliminate the need to choose between IVUS and OCT, now that both modalities are offered with Novasight. The company expects that the system’s increased performance, usability, and quality of images will elevate the entire interventional imaging category of medical devices to a new level. Saving hospitals money over purchasing multiple single modality imaging systems and improving imaging versatility in complex cases (and in turn, improving patient outcomes through the use of intravascular imaging) will likely tip customer decisions to dual imaging. The timing of the team’s accomplishments in evolving the system is optimal, given a big wave in interventional imaging is on the horizon: current guidelines are being updated in the EU to Class 1A for using interventional imaging for complex PCI (percutaneous coronary intervention, a minimally invasive procedure that treats coronary artery disease by improving blood flow to the heart), with North America expected to follow closely behind.
Tom Looby is CEO at Conavi Medical, maker of the Novasight Hybrid™ System, headquartered in Toronto. Darcy Hart is director of optics at Minnetronix Medical, which serves as a single-point provider for medical technology innovation and partners with medical device companies to accelerate breakthroughs in optical systems, fluid and gas management, RF energy, and stimulation and wearable devices.