LOS ANGELES — Over 6.5 million Americans experience chronic wounds — wounds that do not heal after a few months. Almost all such wounds contain bacteria, which, if not detected and removed, can lead to severe infection and resulting complications, including amputation if a limb is involved.
This is especially true for patients with diabetic foot ulcers (open sores), which affects one-third of people with diabetes. Approximately 20% of those who develop a diabetic foot ulcer will require a lower-extremity amputation, according to the American Diabetes Association.
When physicians debride, or clean out, a wound, they remove as much bacteria as possible. However, they face one key limitation — not all bacteria can be seen by the human eye, and some may be missed during the debridement.
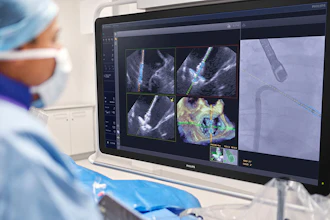
New Keck Medicine of USC research published in Advances in Wound Care suggests there may be a more effective method to detect bacteria during wound debridement. Autofluorescence (AF) imaging, where a handheld device “lights up” bacteria previously invisible to the human eye, uses violet light to illuminate molecules in the cell walls of any bacteria. Different types of bacteria turn different colors, allowing physicians to immediately determine how much and which types of bacteria are in the wound.
“We’re hopeful this new technology can help surgeons improve their accuracy when pinpointing and consequently removing bacteria from wounds and therefore improve patient outcomes, particularly for those with diabetic foot wounds,” said David G. Armstrong, DPM, PhD, a podiatric surgeon and limb preservation specialist with Keck Medicine and senior author of the study. “The early detection and removal of bacteria from a wound is vital to preventing avoidable amputations.”
The research, a literature review of 25 studies examining the effectiveness of AF imaging in treating diabetic patients with foot ulcers, reveals that AF imaging can identify bacteria in wounds in approximately 9 in 10 patients that traditional clinical assessments miss.
Traditionally, physicians debride wounds, then send tissue samples to the lab to identify specific types of bacteria present in the wound and determine the best treatment protocol based on those findings, such as starting the patient on antibiotics or providing a special type of wound dressing. This process can take days, during which time an infection can set in, said Armstrong.
With AF imaging physicians are able to make medical decisions during the wound debridement, rather than waiting for lab results to initiate treatment.
Another benefit to the technology is that if bacteria is caught early, the patient may avoid being prescribed antibiotics, which in wound care can be prolonged, thus avoiding possible antibiotic resistance.
“This real-time intervention may allow for faster, more effective treatment for wounds,” said Armstrong.
Keck Medicine physicians are already using the technology to successfully treat patients with chronic wounds, including diabetic foot ulcers.
“I look forward to more research in this area as we hope to see AF imaging become the standard of care for wound care in the near future,” said Armstrong.
The study is partially supported by the National Institutes of Health, National Institute of Diabetes and Digestive and Kidney Diseases, Award Number 1R01124789-01A1 and the National Science Foundation (NSF) Center to Stream Healthcare in Place (#C2SHiP) CNS Award Number 2052578.