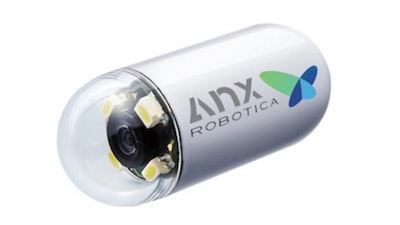
While ingestible video capsule endoscopes have been around for many years, the capsules have been limited by the fact that they could not be controlled by physicians. They moved passively, driven only by gravity and the natural movement of the body. Now, according to a first-of-its-kind research study at George Washington University, physicians can remotely drive a miniature video capsule to all regions of the stomach to visualize and photograph potential problem areas. The new technology uses an external magnet and hand-held video game style joysticks to move the capsule in three-dimensions in the stomach. This new technology comes closer to the capabilities of a traditional tube-based endoscopy.
“A traditional endoscopy is an invasive procedure for patients, not to mention it is costly due to the need for anesthesia and time off work,” Andrew Meltzer, a professor of Emergency Medicine at the GW School of Medicine & Health Sciences, said. “If larger studies can prove this method is sufficiently sensitive to detect high-risk lesions, magnetically controlled capsules could be used as a quick and easy way to screen for health problems in the upper GI tract such as ulcers or stomach cancer.”
More than 7 million traditional endoscopies of the stomach and upper part of the intestine are performed every year in the United States to help doctors investigate and treat stomach pain, nausea, bleeding and other symptoms of disease, including cancer. Despite the benefits of traditional endoscopies, studies suggest some patients have trouble accessing the procedure.
In fact, Meltzer got interested in the magnetically controlled capsule endoscopy after seeing patients in the emergency room with stomach pain or suspected upper GI bleeding who faced barriers to getting a traditional endoscopy as an outpatient.
“I would have patients who came to the ER with concerns for a bleeding ulcer and, even if they were clinically stable, I would have no way to evaluate them without admitting them to the hospital for an endoscopy. We could not do an endoscopy in the ER and many patients faced unacceptable barriers to getting an outpatient endoscopy, a crucial diagnostic tool to preventing life-threatening hemorrhage,” Meltzer said. “To help address this problem, I started looking for less invasive ways to visualize the upper gastrointestinal tract for patients with suspected internal bleeding.”
The study is the first to test magnetically controlled capsule endoscopy in the United States. For patients who come to the ER or a doctor’s office with severe stomach pain, the ability to swallow a capsule and get a diagnosis on the spot – without a second appointment for a traditional endoscopy – is a real plus, not to mention potentially life-saving, says Meltzer. An external magnet allows the capsule to be painlessly driven to visualize all anatomic areas of the stomach and record video and photograph any possible bleeding, inflammatory or malignant lesions.
While using the joystick requires additional time and training, software is being developed that will use artificial intelligence to self-drive the capsule to all parts of the stomach with a push of the button and record any potential risky abnormalities. That would make it easier to use the system as a diagnostic tool or screening test. In addition, the videos can be easily transmitted for off-site review if a gastroenterologist is not on-site to over-read the images.
Meltzer and colleagues conducted a study of 40 patients at a physician office building using the magnetically controlled capsule endoscopy. They found that the doctor could direct the capsule to all major parts of the stomach with a 95 percent rate of visualization. Capsules were driven by the ER physician and then the study reports were reviewed by an attending gastroenterologist who was physically off-site.
To see how the new method compared with a traditional endoscopy, participants in the study also received a follow up endoscopy. No high-risk lesions were missed with the new method and 80 percent of the patients preferred the capsule method to the traditional endoscopy. The team found no safety problems associated with the new method.
Yet, Meltzer cautions that the study is a pilot and a much bigger trial with more patients must be conducted to make sure the method does not miss important lesions and can be used in place of an endoscopy. A major limitation of the capsule includes the inability to perform biopsies of lesions that are detected.
The study, “Magnetically Controlled Capsule for Assessment of the Gastric Mucosa in Symptomatic Patients (MAGNET): A Prospective, Single-Arm, Single-Center, Comparative Study,” was published (insert date) in iGIE, the open-access, online journal of the American Society for Gastrointestinal Endoscopy.
The medical technology company AnX Robotica funded the research and is the creator of the capsule endoscopy system used in the study, called NaviCam®.