Melzi Surgical, a medical device company that helps locate lost surgical sharps, and Spartan Medical, a veteran-owned medical solutions company, have launched a campaign to raise awareness around the impacts of Retained Surgical Items (RSIs) and near-misses to provide a unique offering to reduce RSIs and potential consequences.
RSIs are soft goods (sponges, towels, etc.) and hard goods (instruments, needles, fragments, screws, guidewires, etc.) that are unintentionally left in the patient during surgery. RSIs are one of the top three Joint Commission never-events every year for the last decade. Government data estimates between 4,500 and 6,000 RSIs occur per year with the actual number being unknown1.
Many hospital facilities have experienced a reduction in RSI cases related to soft goods by adopting one of the commercially available sponge detection systems. However, under current established safety protocols, RSI cases relating to hard goods continue to rise, especially due to the increased use of robot-assisted surgeries and the use of smaller instruments and needles2.
It is common practice for operating room nurses to conduct a physical count of all items used during surgery to confirm nothing is missing. Still, miscounts happen in one out of eight cases and counting methods do not cover situations of broken instruments, fragments, screws, or guidewire bits3.
The main contributing factors of RSIs were identified as human factors (distraction, insufficient knowledge), leadership (insufficient policies or compliance) and communication.4 In fact, A root cause analysis report by the Veterans Health Administration (VHA) on its 1.5 million safety reports showed that intravascular loss of guidewires is an act of omission error, a concept that some steps are prone to be missed because they require memory and attention after the completion of the main goal5.
Upon discovery of a miscount, the current recommended protocol from the Association of Perioperative Registered Nurses (AORN) is to call for an X-ray. However, an X-ray typically takes 25 to 30 minutes to arrive and another 20 to 30 minutes to take the films for analysis6.
On average, the entire process takes 45 minutes and is only 25% to 50% effective6. The use of X-ray for suspected RSIs results in prolonged anesthesia time for the patient, exposes both the patient and OR team to additional ionizing radiation, and potentially derails and delays the current case and subsequent procedures.
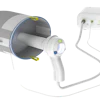
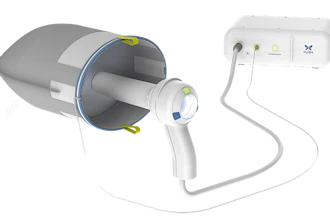
Since FDA approval, risk managers and several hospital systems began adopting the Melzi Sharps Finder (MSF) as part of their RSI prevention protocol. When a miscount situation happens, the MSF locates the missing item inside the patient's body within minutes. The video below show a lost sharps in a patient and how the Melzi Sharps Finder quickly locates a lost needle.
In a lab study, testing results with the Melzi Sharps Finder show detection of 13mm, 17mm, and 26mm needles with a 95% reliability rate7. The Melzi Sharps Finder is a hand tool capable of being deployed through a 5mm trocar for laparoscopic and robotic surgeries and can also be used in open surgery.
The use of an adjunct technology, like the Melzi Sharps Finder, can enhance patient safety, save time, and reduce overall risks. The MSF is an FDA-registered single-use, sterile device that can be used in-vivo and detect lost needles, consistently as small as 7.0mm8.
Citations:
- Goodwin, B. JD, RN (2018, March 1). Retained surgical lawsuits will cost you. Retrieved from Urology Times: https://www.urologytimes.com/view/retained-surgical-item-lawsuits-will-cost-you
- Weprin, S. A., Moore, R. H., Meyer, D., & Autorino, R. (2020). Retained Surgical Items: a changing landscape. Journal of Patient Safety, 17(1), e41. https://doi.org/10.1097/pts.0000000000000777
- Weprin, S., Crocerossa, F., Meyer, D., Maddra, K., Valancy, D., Osardu, R., Kang, H. S., Moore, R. H., Carbonara, U., Kim, F. J., & Autorino, R. (2021). Risk factors and preventive strategies for unintentionally retained surgical sharps: a systematic review. Patient Safety in Surgery, 15(1). https://doi.org/10.1186/s13037-021-00297-3
- Steelman, V. M., Shaw, C., Shine, L., & Hardy-Fairbanks, A. J. (2019). Unintentionally Retained Foreign Objects: A descriptive study of 308 sentinel events and contributing factors. The Joint Commission Journal on Quality and Patient Safety, 45(4), 249–258. https://doi.org/10.1016/j.jcjq.2018.09.001
- Cherara, L., Sculli, G. L., Paull, D. E., Mazzia, L., Neily, J., & Mills, P. D. (2018). Retained guidewires in the Veterans Health Administration: getting to the root of the problem. Journal of Patient Safety, 17(8), e911–e917. https://doi.org/10.1097/pts.0000000000000475
- Autorino, R. MD (2021, April 3). Incidence and OR team awareness of "near-miss" and retained surgical sharps: a national survey on United States operating rooms. Retrieved from Patient Safety in Surgery: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC8019169/
- Out of the box 13mm, 17mm, and 26mm needles are detected at 95% reliability with 95% confidence, 9mm and 11mm needles with greater than 80% reliability @ 90% confidence, and 6mm needles with 70% reliability @ 90% confidence. Additionally, when magnetized by placing an individual needle on a magnetic instrument mat for 1 second (verified using Key Surgical MG-300-400R instrument mat ) all the previously listed needle groups: 6mm, 9mm, 11mm, 13mm, 17mm and 26mm are detected at 95% reliability with 95% confidence.
- J, Adams, Ph.D., J Noel, Ph.D. (2022) Needle Size and Detectability Study.